Arbovirus surveillance
Project coordinator: Somphavanh Somlor
Member of staff: Thonglakhone XAYBOUNSOU, Phaithong Bounmany, Sitsana Keosenhome
Funded by the International Division, Institut Pasteur, Paris In collaboration with the Arbovirus and vectors unit and Pathogen Genotyping Pole, Institut Pasteur, Paris.

Blood collection in Phonephapao Factory
Background:
Dengue is considered as the main vector-borne disease causing severe mortality and morbidity in the Lao PDR. Before 2010, dengue surveillance was mostly based on syndromic surveillance. Since 2012, the Institut Pasteur du Laos is monitoring dengue in Vientiane Capital through a laboratory-based surveillance network. Additional Lao provinces, Saravanh and Attapeu, accessed the network in 2015 as requested by the Lao Ministry of Health. Evidence-based results from this surveillance serve as reference for prevention and control strategies. New approaches are now in development with the help of experts in data modeling to improve alert capacities but also to anticipate epidemiologic modification of dengue transmission in the evolving urban environment of Vientiane Capital.
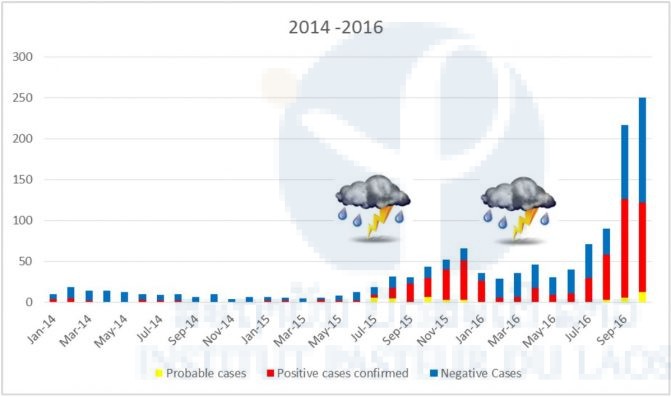
Trends of dengue circulation in Vientiane Capital, Saravanh and Attapeu 2015–16
For the second consecutive year, a shift of several weeks in the peak of dengue transmission has been observed. This particular profile was a probable consequence of low rainfall during the expected rainy season (April–September) and delayed precipitations that occurred in late August 2016. The 2016 surveillance evidenced a new change in dengue serotype predominance with the extension of DENv-4. Of the three provinces observed by IPL, a predominance of DENv-4 has been observed. The risk of outbreak has been anticipated because, as in 2012–13, this serotype emerged in Vientiane Capital and circulated during the dry season.
Mapping of dengue cases in Vientiane Capital
To better understand the dynamics of dengue in Vientiane Capital, IPL started collecting GPS coordinates for the dwellings of dengue confirmed cases. This mapping now allows identifying, in a timely manner, dengue occurrence hotspots, establishing the dynamic of dengue transmission and comparing the current profile to the previous years (Figure 4).
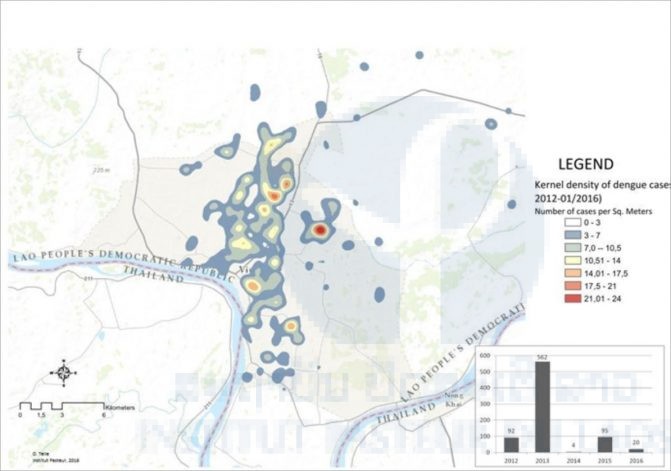
Figure 4: Distribution of dengue confirmed cases in Vientiane Capital 2012–2016
Since July 2015, two additional provinces, Saravanh and Attapeu, were included in the IPL dengue surveillance network upon the request of the Lao Ministry of Health. Transportation systems in place with these two provinces demonstrated their efficacy in terms of minimal delivery delay and preservation of the samples for diagnosis purposes. Data from these provinces highlight the complexity of dengue transmission at a national scale. If DENv-4 was found as the major serotype circulating in the three provinces covered by IPL network, local specificities were evidenced. In Saravanh, a low level of DENv-1 and DENv-3 has been recorded. Only DENv-4 has been detected in Attapeu as a possible consequence of a lower number of samples collected. In Vientiane Capital DENv-4 was predominant, followed by DENv-1. DENv-2 has also been detected at the origin of a “micro-epidemic” that occurred in a factory where workers from the provinces are accommodated. Introduction of DENv-2 in this micro-environment was probably linked to an imported case from an other province.
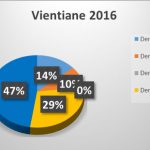
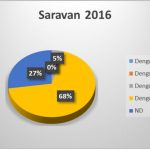

Figure 5: Distribution of dengue serotypes in the three provinces participating in the IPL dengue surveillance network. (A) Vientiane Capital; (B) Saravanh; (C) Attapeu.
Zika virus surveillance
Since 2015, the Zika virus has been included in the differential diagnosis process of dengue suspected cases. Different RT-PCR protocols were tested on reference Zika strains (prototypes of African and Asian genotypes) and on a panel of human plasma. No case of Zika virus could be identified so far. Following international comsensus on Zika virus diagnosis indicating the high sensitivity of urine testing, recommendations were rapidly sent to the clinicians’ network to systematically collect urine samples from dengue suspected cases. The diagnostic algorithm has been adapted to integrate this new biological fluid into the diagnostic process. Until now, no acute Zika virus infection has been detected in Vientiane Capital.
Seroprevalence studies are ongoing to determine the level of exposure of Lao populations to Zika virus in different provinces (cf. R&D section).
“Kinetic study of cellular viremia of dengue virus in Vientiane Capital, Lao PDR” Research program PTR-491
Funded by the International Division, Institut Pasteur, Paris In collaboration with the Arbovirus and vectors unit and Pathogen Genotyping Pole, Institut Pasteur, Paris.
Project coordinator: Somphavanh Somlor
Member of staff: Thonglakhone XAYBOUNSOU, Phaithong Bounmany and Sitsana Keosenhome
Background:
Dengue viruses can be efficiently isolated from peripheral blood mononuclear cells. Scientific reports and internal laboratory experience confirmed the importance of this procedure, especially when plasmatic viremia is negative. However, precise knowledge on the kinetic of dengue cellular viremia is missing to potentially integrate this method in dengue virus diagnostic algorithm. A specific study has been set up to establish the duration of dengue cellular viremia with two different components: (i) a retrospective study on dengue suspected cases included between 2012 and 2015 to compare plasmatic and cellular dengue viremia and (ii) a prospective longitudinal study on confirmed cases to establish the kinetic of the two types of dengue viremia.
Altogether, a total of 452 dengue confirmed cases, 264 cases and 188 cases respectively for the retrospective and prospective studies, could be investigated. The distribution of the different markers is now analyzed in order to establish their kinetic and to determine the contribution of cellular dengue viremia detection to dengue infection direct diagnosis. Differences between serotypes will also be studied as samples for all four dengue serotypes are available for the retrospective study. As shown in Figure 6, only samples from patients infected by serotypes 1, 2, and 4 are available at present as DENv-3 has not circulated in Vientiane Capital since December 2013.
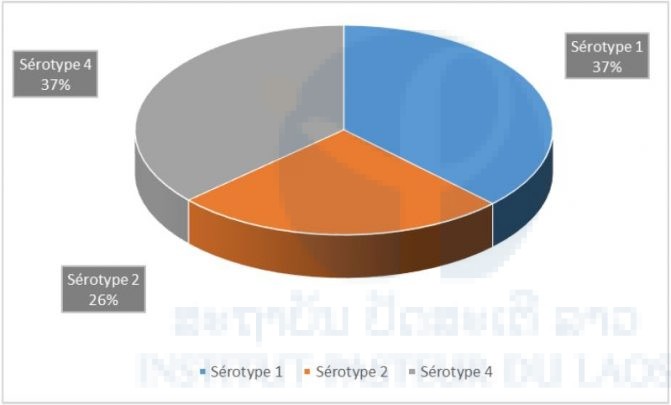
Figure 6: Proportion of the different dengue serotypes among patients who were the subject of a follow up in 2015–16.