Investigation of the etiology of undifferentiated febrile syndromes through an integrated virological/ entomological/high-throughput sequencing approach to map the circulation of arboviruses, rickettsioses and other intracellular bacteria in humans and vectors in Lao PDR.
 Collaboration
Collaboration
Medical Entomology Laboratory, IPL, Lao PDR.
Funding
• Ministry of Higher Education, Research and Innovation, France.
Objectives
The global objective is to investigate the causes of undifferentiated febrile syndromes in Lao PDR using an integrated virological and entomological approach. This project aims to map the circulation of arboviruses, rickettsioses, and other intracellular bacteria in humans and vectors by screening blood samples collected during the acute phase from patients presenting with “denguelike” fever who had previously tested negative for Dengue virus (DENV), Chikungunya virus (CHIKV), and Zika virus (ZIKV).
Background
At the request of the Lao Ministry of Health (MOH), IPL has developed surveillance of arboviruses in the country, currently focused on DENV, CHIKV and ZIKV infections. This surveillance has extended to 22 civil and military hospitals, spread across ten provinces in Lao PDR. At the same time, several entomological study programs on mosquitoes, sandflies, and ticks have been developed. Currently, 40 to 50% of arbovirus surveillance blood samples tested at IPL were negative for DENV, CHIKV, and ZIKV. This suggests that other pathogens causing “dengue-like” febrile syndromes, such as those from the Alphavirus, Flavivirus, and Phlebovirus genera, may also be circulating in Lao PDR.
Pan-alphavirus, pan-fl antivirus, and pan-phlebovirus molecular detection assays have previously been validated by the Medical Entomology Laboratory to detect the presence of these viruses in vectors, such as mosquitoes, sandflies, and ticks. These techniques were used on blood samples taken during the febrile phase from patients clinically suspected of dengue fever, in which virological analyses are negative for DENV, CHIKV, and ZIKV.
Rickettsioses are infectious diseases caused by obligate intracellular gram-negative bacteria. They belong to the order Rickettsiales and reside in a wide range of arthropod vectors, such as fleas, ticks, and mites.
This project was structured, in collaboration with the Medical Entomology Laboratory, around three main axes: 1) detection of arboviruses, rickettsia, and other intracellular bacteria in humans; 2) detection of arboviruses, rickettsia, and other intracellular bacteria in vectors; 3) precise identification and molecular characterization by high-throughput sequencing of the detected pathogens. Here, only the results on the first axis will be presented. The results of the second and third axes will be presented by the Medical Entomology Laboratory.
Methodology
Sample selection
Samples were selected from the IPL arboviruses surveillance biobank in 2023 and 2024. Briefly, in 2023, among the 2519 samples tested at IPL, 853 were negative for DENV, ZIKV, and CHIKV (see next paragraph), and between January and September 2024, 125 were negative among the 196 samples tested. Among these 978 samples that tested negative for DENV, ZIKV, and CHIKV, 761 were selected for arbovirus screening and 709 for the rickettsia screening based on the availability of biological materials (extracted RNA for arboviruses screening and buff y coat for rickettsia screening) and their geographical representativeness. The geographical origin of the samples is shown (Figure 1).
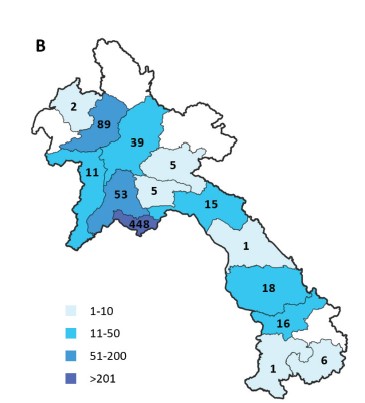
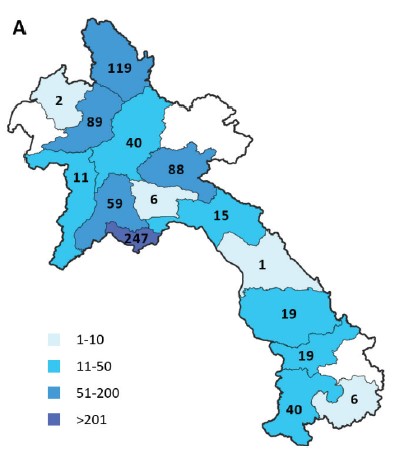
Figure 1: Origin of samples for arbovirus (A) and rickettsia (B) detection.
DENV, ZIKV and CHIKV detection
Virus nucleic acids are extracted from human plasma by Nucleo Spin RNA virus kit (Macherey-Nagel), Nucleo Spin 8 virus kit (Macherey-Nagel), or Nucleic Acid Extraction Rapid kit (Bioperfectus) according to the manufacturer’s instructions. Extracted RNAs are then screened for the presence of dengue (DENV) and Zika (ZIKV) viruses by a duplex one-step real-time RT-PCR assay. The plasma samples that test negative for DENV by PCR are screened by the Dengue NS1 Antigen + Antibodies Combo rapid test (SD Bioline) for detection of DENV NS1, anti-DENV IgM, and anti-DENV IgG. Finally, samples that test negative for DENV by PCR and/or DENV NS1 by rapid test are then screened for the detection of chikungunya virus (CHIKV) using a real-time RT-PCR assay.
Arbovirus detection
Extracted RNAs from samples that tested negative for DENV by PCR and/or DENV NS1 and/or anti-DENV IgM and ZIKV and CHIKV by PCR are reverse-transcribed to complementary DNA (cDNA) by Maxima H Minus First Strand cDNA Synthesis Kit (Thermo Fisher Scientific) according to the manufacturer’s instructions. cDNAs are then screened by pan-alphavirus, pan-fl avivirus, and pan-phlebovirus nested PCR.
Rickettsia detection
Nucleic acids are extracted from a human buff y coat by Nucleo Spin 8 virus kit (Macherey-Nagel) according to the manufacturer’s instructions, with a proteinase K treatment. Extracted DNAs are then screened by i) one probe-based real-time qPCR assay to detect O. tsutsugamushi (47 kDa htrA gene) (2) and ii) i) two probe-based real-time qPCR assays to detect Rickettsia genus (17 kDa gene) (2,3).
Rickettsia species identification
Seventeen kDa real-time PCR-positive samples are subsequently screened with a panel of nested conventional PCR assays targeting the 17 kDa, gltA, ompB, ompA, and sca4 genes. For positive amplicons, DNA sequencing was done using a BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems) on a 3500xL Genetic Analyzer apparatus (Applied Biosystems). The raw sequences are analyzed and edited using Unipro UGENE software, and then the identification of the species is performed by using the Nucleotide Basic Local Alignment Search Tool (BLAST-N) implemented in the NCBI website (https:// blast.ncbi.nlm.nih.gov/blast/Blast.cgi).
Results
Arbovirus detection
No viruses were detected among the 761 samples screened by the nested PCR assays to detect Alphavirus, Flavivirus, and Phlebovirus genera arboviruses.
Rickettsia detection
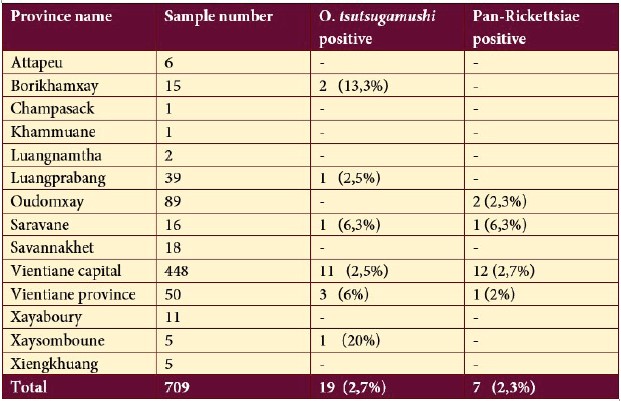
Among the 709 selected samples, O. tsutsugamushi was detected in 19 samples (2.7%), and the presence of the Rickettsia genus was detected by at least 1 of the two qPCR systems in 16 samples (2.3%). O. tsutsugamushi was detected in samples originating from 6 provinces: Borikhamxay (n=2), Luangprabang (n=1), Saravane (n=1), Vientiane Capital (n=11), Vientiane (n=3) and Xaysomboune (n=1); whereas Rickettsia was detected in samples originated from 4 provinces: Oudomxay (n=2), Saravane (n=1), Vientiane Capital (n=12), Vientiane (n=1) (Table 1). No coinfection was detected among the positive samples.
Table 1: Molecular assay results of Rickettsia detection.
In order to identify the Rickettsia species, positive samples were subsequently screened with a panel of nested conventional PCR assays targeting the 17 kDa, gltA, ompB, ompA, and sca4 genes.
Eight amplicons were obtained using the 17kDa nested- PCR assay. Based on the Sanger sequences, five samples are found to be genetically close to R. typhi (the agent of murine typhus, transmitted by fleas) and 1 sample to R. felis (the agent of flea-borne spotted fever or cat-flea typhus, transmitted by fleas). For the two other samples, the species could not be conclusively identified due to the small size of the PCR products.
Discussion
No viruses were detected among the 761 samples screened using nested PCR assays targeting the Alphavirus, Flavivirus, and Phlebovirus genera of arboviruses. The negative results from human samples suggest the need for further improvements. This could involve either (i) optimizing the existing detection systems to enhance their sensitivity or (ii) developing new detection assays that specifically target arboviruses known to infect humans in Southeast Asia.
Among the 709 samples selected for Rickettsia screening, Orientia tsutsugamushi was detected in 19 samples (2.7%), and the presence of the Rickettsia genus was confirmed in 16 samples (2.3%). No coinfections were observed among the positive cases. Of the 16 Rickettsiapositive samples, the species were identified in 6 cases: 5 samples were genetically similar to R. typhi (the causative agent of murine typhus, transmitted by fleas), and 1 sample to R. felis (the causative agent of fleaborne spotted fever or cat-flea typhus, also transmitted by fleas). Further identification of the Rickettsia species in the remaining samples will be pursued using a panel of nested conventional PCR assays targeting the 17 kDa, gltA, ompB, ompA, and sca4 genes.
These results confirmed the circulation of O. tsutsugamushi (the agent of the scrub typhus, transmitted by mites) and R. typhi and R. felis in Lao PDR, as previously reported. A prior study found these three Rickettsiae to be present in 2.6% to 14.8% of febrile syndromes (1). However, the detection rates of Rickettsiae in our study are lower than those reported in a 2006 study that used serological methods, which may explain the discrepancy. Our findings are more consistent with a 2013 study conducted in Luangnamtha and Saravane provinces. That study, using molecular techniques combined with culture, detected O. tsutsugamushi (7%), R. typhi (<1%), undetermined Rickettsia species, and R. felis (<1%) among blood samples from 1,938 patients with febrile syndromes (4).
Other bacteria associated with undifferentiated fevers in humans have already been identified in ticks in Lao PDR, including Anaplasma phagocytophilum (the agent of anaplasmosis) and Borrelia spp. (the agents of borreliosis, the most well-known of which is Lyme disease), Coxiella burnetii (the agent of Q fever) and Ehrlichia chaffeensis (the agent of human monocytic ehrlichiosis) (5). Although some of these diseases have not yet been reported in Lao PDR, the identification of their causative agents in local vectors suggests that it would be valuable to test for their presence in human samples.
Conclusion & perspectives
This study did not identify arboviruses of the Alphavirus, Flavivirus, and Phlebovirus genera in blood samples taken during the febrile phase from patients clinically suspected of dengue fever, in 2023 and 2024, in which the virological tests are negative for DENV, CHIKV, and ZIKV, suggesting a need to optimize these assays. Performing a virome analysis using next-generation sequencing (NGS) on a subset of samples from patients in the febrile phase, where the causative agent of the febrile syndrome could not be identified in this study, may facilitate the detection of new arboviruses. This approach could potentially lead to the development of specific detection systems that could be used for screening human samples in the future.
Finally, this study confirms that several rickettsioses, such as scrub typhus, murine typhus, or tick-borne spotted fever, can be responsible for “dengue-like” fever in Lao PDR, which has significant public health implications. While there is no specific antiviral therapy for dengue fever, rickettsioses necessitate appropriate antibiotic treatment. Therefore, the investigation of these rickettsioses as potential differential diagnoses for dengue fever should be prioritized in the Laotian context.
References
1. Phongmany S, Rolain JM, Phetsouvanh R, Blacksell SD, Soukkhaseum V, Rasachack B, et al. Rickettsial infections and fever, Vientiane, Laos. Emerg Infect Dis. 2006 Feb;12(2):256–62.
2. Jiang J, Chan TC, Temenak JJ, Dasch GA, Ching WM, Richards AL. Development of a quantitative real-time polymerase chain reaction assay specific for Orientia tsutsugamushi. Am J Trop Med Hyg. 2004 Apr;70(4):351– 6.
3. Jiang J, Stromdahl EY, Richards AL. Detection of Rickettsia parkeri and Candidatus Rickettsia andeanae in Amblyomma maculatum Gulf Coast ticks collected from humans in the United States. Vector Borne Zoonotic Dis. 2012 Mar;12(3):175–82.
4. Mayxay M, Castonguay-Vanier J, Chansamouth V, Dubot-Pérès A, Paris DH, Phetsouvanh R, et al. Causes of non-malarial fever in Laos: a prospective study. The Lancet Global Health. 1(3):e46. 5. Taylor AJ, Vongphayloth K, Vongsouvath M, Grandadam M, Brey PT, Newton PN, et al. Large-Scale Survey for Tickborne Bacteria, Khammouan Province, Laos. Emerg Infect Dis. 2016 Sep;22(9):1635–9.