Tetanus and diphtheria seroprotection in Lao adolescents

Collaboration.
Lao Tropical and Public Health Institute; Luxembourg Institute of Health.
Funding.
Ministry of Foreign and European Affairs, Luxembourg Luxembourg Institute of Health, Luxembourg.
Objectives.
Investigating the seroprevalence and protective levels of antibodies against diphtheria and tetanus among Lao adolescents in Vientiane Capital and Bolikhamxay province.
Background.
Diphtheria, caused by Corynebacterium diphtheriae, usually spreads from person-to-person by droplets. The typical clinical manifestation is pseudo-membranous pharyngitis and the disease has a mortality rate of 5-10%. Tetanus occurs following infection with toxigenic strains of the bacterium Clostridium tetani, mainly via broken skin or in mothers and neonates during/shortly after childbirth due to unclean birth practices or cord care. The toxin causes motor neuron hyperactivity, hypertonia and muscle spasms resulting in high morbidity and mortality in the absence of medical intervention.
Diphtheria and tetanus vaccines are important during childhood, typically given in combination and with or without other vaccines. The World Health Organisation (WHO) recommends three doses of diphtheria and tetanus vaccines in the first 12 months of life and three further booster doses before adolescence. Women of childbearing age are also included in tetanus vaccination schedules to protect both the mother and newborn against Maternal and Neonatal Tetanus (MNT). The WHO recommends providing booster doses to women of reproductive age who have not yet received six doses.
In the Lao People’s Democratic Republic (Lao PDR), MNT elimination – i.e. less than one case per 1000 live births – was achieved in 2014 [5]. Diphtheria and tetanus vaccinations are part of the pentavalent vaccine (diphtheria-tetanus-pertussis-hepatitis B-Haemophilus influenzae; DTP-HepB-Hib) scheduled at 6, 10 and 14 weeks of age. Coverage estimates differ by source: for example, in 2017 the coverage of the third dose of DTP-HepB-Hib vaccine was 58.8% according to the Lao Social Indicator Survey whereas the government estimate reported to the WHO was 85% for the same year. The WHO-recommended boosters for tetanus and diphtheria vaccines before the age of 15 are not routinely given in Lao PDR.
Reporting health data is challenging in Lao PDR. Although reports of tetanus are rare, previous studies have suggested low immunity in male Lao adolescents and missed opportunities to vaccinate pregnant women during antenatal care. Furthermore, in 2017 less than half of Lao women of childbearing age were estimated to be protected against tetanus. More than 100 cases of diphtheria were reported in 2012/13 and in 2015 in Lao PDR, likely due to low vaccination coverage and/or suboptimal vaccine immunogenicity.
The aim of this study was to determine the seroprevalence and protective levels of antibodies against diphtheria and tetanus among Lao adolescents in Vientiane Capital and Bolikhamxay province, thereby including urban and rural areas, and to provide evidence-based data to policymakers regarding the need for booster vaccinations.
Methodology
Serum samples from 779 adolescents collected in the framework of a randomized cross-sectional hepatitis B serology study in 2018 were utilized in this study. Randomly selected students aged between 11 and 18 years from schools in Vientiane Capital and Bolikhamxay province (Paksan and Pakkading districts) were asked to participate. All students and their guardians were asked for their consent and were informed that they could withdraw at any time.
The study was approved by the Lao National Ethics Committee (Nr 022/NECHR) and the Institutional Review Board of the Institut Pasteur du Laos (Nr 9).
Samples were tested with commercial ELISA kits (Euroimmun) to determine IgG antibody levels against diphtheria and tetanus according to the manufacturer’s instructions.
Anti-tetanus titers were grouped into “Insufficient immunity, booster vaccination recommended” (<0.1 IU/ ml), “Immunity given, booster vaccination will provide long-term immunity” (0.1-0.5 IU/ml), “Sufficient immunity, booster vaccination in 2-5 years” (>0.5-1.1 IU/ml), “Sufficient immunity, booster vaccination in 5-10 years” (>1.1-5.0 IU/ml) and “Sufficient immunity, booster vaccination in approximately 10 years” (>5.0 IU/ml). Out of all samples, 49 serum samples had an anti-tetanus titer exceeding the detection limit of the ELISA kit and were tested again in dilution (1:400). After retesting, anti-tetanus IgG titers of 12 samples remained above the detection limit and were not retested.
Results
Population characteristics
Most of the participants were of Tai-Kadai ethnicity (Vientiane Capital: 98%; Bolikhamxay province: 93%). The median age of the participants was 15 years and 49% were male (Vientiane Capital: 47%, Bolikhamxay province: 51%).
Seroprevalence of diphtheria IgG antibodies
Overall, 25.8% of participants had anti-diphtheria IgG antibody titers≥0.1 IU/ml, indicating immunization protection. Most of the participants (69.1%) had antibody levels corresponding to “uncertain protection”. We observed differences in the proportion of participants protected against diphtheria according to age, sex and type of nearest healthcare facility (Figure 1). Age and anti-diphtheria titer were positively correlated among female participants (rho=0.3; p<0.0001), but not among male participants (rho=-0.02; p=0.673).
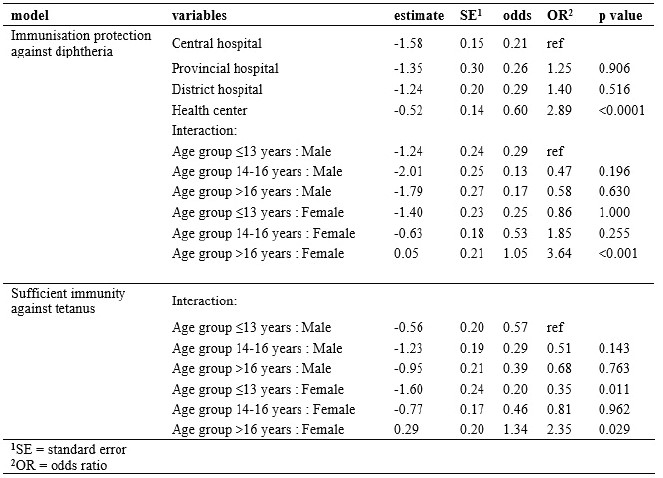
In bivariate analysis, female participants, participants older than 16 years, participants recruited in Bolikhamxay province, or especially in Pakkading district, and participants whose closest health facility was a health center were more likely to be protected. The variables “province”, “district” and “nearest health care facility” were highly correlated with each other: most students recruited in Vientiane Capital lived close to a Central hospital while most students recruited in Pakkading, a rural area, lived closest to a health center. The best fitting model included the variables “sex”, “age” and “nearest health care facility”; and an interaction between sex and age. Post-hoc analyses of the final model were conducted, resulting in adjusted model estimates (Table 1). Female participants older than 16 years and living closest to a health center were significantly more likely to be protected against diphtheria (p<0.0001) compared to males ≤13 years of age (p<0.0001). Participants living closest to a health center were also more likely to be protected (p<0.0001) compared to participants living closer to a Central hospital (p<0.0001).
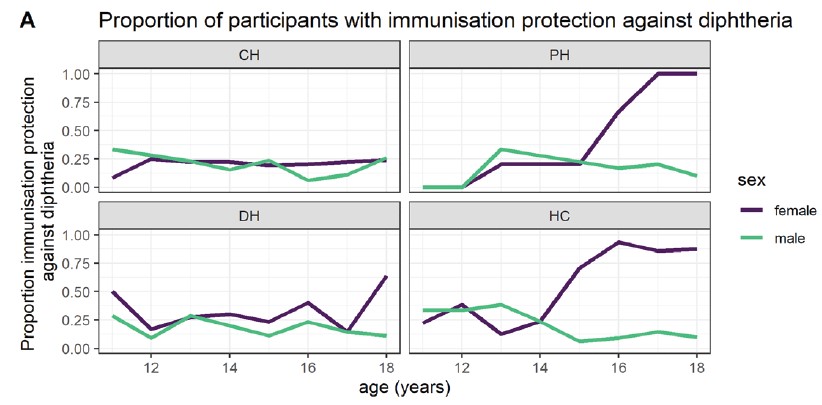
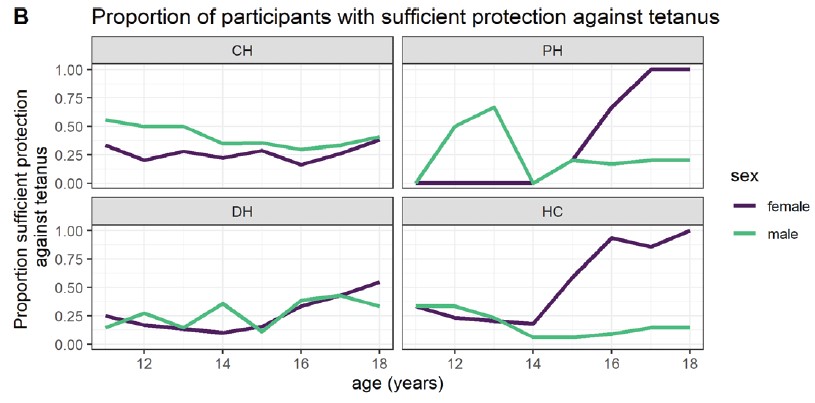
Figure 1. The proportion of participants with immunization protection against diphtheria (A) and sufficient immunity against tetanus (B) according to age and stratified by sex and nearest health care facility. CH = central hospital, PH = provincial hospital, DH = district hospital and HC = health center.
Table 1. Model estimates after post-hoc analyses of binomial generalized linear model for immunization protection against diphtheria and for sufficient immunity against tetanus.
Seroprevalence of anti-tetanus IgG antibodies
In total, 30.9% of participants had an anti-tetanus IgG titer >0.5 IU/ml corresponding to “sufficient immunity” (Table 1). Serological profiles were relatively similar at both study sites: the proportion of participants with sufficient immunity was 31.7% in Vientiane Capital and 30.2% in Bolikhamxay province.
Age and anti-tetanus titer were positively correlated in female participants (rho=0.23; p<0.0001) and negatively in males (rho=-0.14; p<0.008). against tetanus.
When the proportion of sufficiently protected participants was plotted according to age and stratified by sex and nearest healthcare facility, the observed pattern was similar to the anti-diphtheria data: a higher proportion of older female students living closest to the provincial hospital or a health center were protected as compared to younger males (Figure 1).
In bivariate analysis, age and sex were associated with being sufficiently immune and both variables were included in the logistic regression model. There was a significant interaction between the two variables, indicating that the protection against tetanus by age depends on the sex of the participants and vice versa. In post-hoc analyses, when all possible participant groups were compared to males ≤13 years, female participants ≤13 years were 0.35 times less likely to have sufficient immunity against tetanus (p=0.01) (Table 1). Female participants >16 years were 2.4 times more likely to have sufficient immunity (p<0.029).
Discussion
In this study, we found low rates of sufficient immunization protection against tetanus and diphtheria among Lao adolescents from Vientiane Capital and Bolikhamxay province.
The proportion of participants with sufficient levels of antibodies against diphtheria was only 26% (compared to around 50% in a study from Thailand). A low diphtheria seroprotection is concerning and may indicate susceptibility in younger ages where the disease is more severe. Indeed, although the number of reported cases in Lao PDR has decreased since the introduction of the vaccine in infants, the WHO reported 73 cases in 2019 and a study of outbreaks in 2012/2013 found a median age of 10.5 years.
In the current study, the seroprotection increased significantly with age in female participants. This increase with age for anti-diphtheria, as well as for antitetanus antibodies, was strongest in those women whose closest health facility was a Provincial hospital or a health center, maybe reflecting better vaccination coverage in those locations.
The overall protection against tetanus was 30.9% and lower in male adolescents (28%) than in females (34%). Although females have the risk of MNT, adolescent and adult males have other routes of exposure such as from contaminated wounds, and men make up a large proportion of cases in low-income countries. Indeed, even in those few protected males in the current study, lower antibody levels were seen with increased age underlining the high susceptibility of adult males.
Although females had higher overall protection against tetanus, the younger adolescent girls had a slightly lower chance of being protected than the boys. However, protection in the girls increased significantly with age and those >16 years were more likely protected than young girls. This is likely to be due to the policy to vaccinate females aged 15-49 with tetanus-containing vaccines and thereby reducing the risk of MNT. The introduction of tetanus/ diphtheria combined vaccine (Td) within the last 10 years also explains the similar increase in diphtheria antibody titers in older female adolescents. MNT was eliminated from Lao PDR according to a validation study in 2013 due to a concerted effort by the Lao Ministry of Health to vaccinate women of reproductive age and to improve birth practices and umbilical cord care. Here, although we see that the policy resulted in an increased seroprotection of adolescent females, a substantial proportion (66.4%) were still not sufficiently protected (titers <0.5 IU/ml). This compares to less than 5% with these antibody levels in a study in neighboring Thailand, where boosters – for males and females – are implemented at the age of 18 months and 4-6 years and are recommended at 11- 12 years of age and every 10 years thereafter. In 2017 in Vientiane Capital and Bolikhamxay province, only 49.4% and 55.9% of women of child-bearing age were estimated to be protected against tetanus, indicating a need to strengthen the existing vaccination policy. Furthermore, in Lao PDR, there are still a large number of young pregnancies, especially in rural areas, where females younger than 15 years of age would benefit from a booster vaccination.
A limitation of the current study was that we did not have access to the vaccination history of the participants. Therefore, the reason for low tetanus and diphtheria seroprotection could be either low vaccination coverage waning of vaccine-induced antibodies or both or low immunogenicity. Also, the data should be extrapolated nationwide with caution as the study only took place in two provinces.
Conclusion & perspectives
Taken together with our previous observations of missed opportunities to vaccinate during early ANC visits, these data suggest a strengthening of tetanus and diphtheria vaccination coverage and booster doses in females before or during adolescence should be considered to maintain elimination of MNT and reduce susceptibility to diphtheria infection. The Lao Ministry of Health should also review the burden of tetanus and diphtheria in adolescent and adult males and consider Td vaccination boosters before adolescence.
The results were communicated as a policy brief to the Lao National Immunization Programme. A manuscript has been published in Tropical Medicine and International Health journal.