An age-stratified serosurvey against purified Salmonella enterica serovar Typhi antigens in the Lao People´s Democratic Republic
 Project Coordinator: Lisa Hefele, Siriphone Virachith, Antony Black
Project Coordinator: Lisa Hefele, Siriphone Virachith, Antony Black
Collaborating institutions: Wellcome Trust Major Overseas Programme, Oxford University Clinical Research Unit, Ho Chi Minh City, Vietnam, Luxembourg Institute of Health
Publications and communications: Presentation at the Typhoid vaccine stakeholder meeting, Vientiane (with MOH, WHO, GAVI); Manuscript submitted for publication.
Background
Typhoid fever is a systemic disease caused by the bacterium Salmonella enterica, subspecies enterica serovar Typhi (S. Typhi) and is transmitted through contaminated food or water. Blood culture is regarded as the gold standard for the diagnosis of typhoid fever, but it is less sensitive than the more invasive bone marrow culture and requires the necessary laboratory capacities, which poses a challenge for many countries.
As an alternative, the serology-based Widal test is another method for the diagnosis of typhoid fever, although its utilization remains controversial. Due to the inadequate performance of the currently used diagnostic tests, the search for novel methods is ongoing.
The investigation of serological markers for typhoid fever prevalence may aid in overcoming diagnostic challenges and provide estimates of subclinical typhoid fever infections. A number of potential biomarkers have been proposed in previous research works. The antigens hemolysin E (HlyE) and cytolethal distending toxin subunit B homolog (CdtB) are expressed in S. Typhi and S. Paratyphi A, but only rarely in other Salmonella spp. Both antigens are considered to be immunogenic upon S. Typhi infection. Anti-HlyE IgG and anti-CdtB IgG have been previously suggested to be useful biomarkers in distinguishing typhoid fever cases from non-typhoid fever cases. Other studies focus on antibody responses against the immunogenic polysaccharide capsular Vi “virulence” antigen (anti-Vi) which presents the prime target for vaccine development. The Vi antigen is only present in S. Typhi, S. Dublin and S. Paratyphi C, but is absent from S. Paratyphi A and most of the gastroenteritis causing serovars.
In the Lao PDR, typhoid fever is a notifiable disease. Cases of typhoid fever are reported to the National Center for Laboratory and Epidemiology in Vientiane. However, access to health care is still inadequate especially in remote areas and the capacity for blood culture testing in Lao PDR is limited to only three laboratories in the whole country. Currently, the requirements for adequate typhoid fever surveillance are not given which hinders an assessment of disease burden in Lao PDR. The lack of data also impeded recent considerations of including a typhoid fever vaccine into the national immunization schedule. Therefore, typhoid fever vaccination is not part of the national immunization schedule in the Lao PDR.
In order to contribute to the understanding of typhoid fever epidemiology in Lao PDR, we conducted a serological, cross-sectional study using existing serum samples from different age groups and areas of Lao PDR. This study is the first serology-based study in Lao PDR and provides initial insights into age-related exposure to S. Typhi and baseline antibody titers against the HlyE, CdtB and Vi antigen in the general population.
Methods
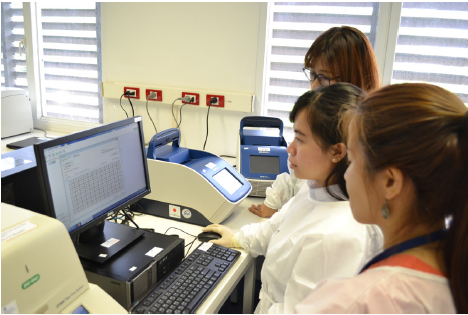
ELISAs were performed on 937 serum samples (317 children and 620 adults) from across Lao PDR to measure IgG antibody titers against Vi polysaccharide and the experimental protein antigens, CdtB and HlyE.
A commercial ELISA kit (Vacczyme, Binding site, UK) was used for determining the anti-Vi IgG antibody responses. Antibody concentrations were derived from the optical density (OD) data using a standardized curve fitting 4-parameter logistic method. Any sample below the calculation limit of the assay was classified as “left censored” for the purpose of analysis. In-house ELISAs were performed to determine anti-HlyE IgG and anti- CdtB IgG levels in the two stud populations.
Statistical analyses were performed in R. Non-parametric statistical tests were employed as appropriate. The relationship between age and antibody levels was assessed by fitting generalized additive models or an Akritas– Theil–Sen non-parametric regression estimation to the data.
Results
Study population
Sera from 317 children and 620 adults were included in the study. The majority of children in the child cohort were from Vientiane (249/317; 78.6%) and most (171/317; 53.9%) were female. The age of the children ranged from 0 to 15 years, with a median age of 8 years. The majority (373/620; 60.2%) of the adult participants were male and over a third (232/620; 37.4%) were students. The age of the adult participants ranged from 17 to 40 years (median 26 years).
The seroprevalence of anti–S. Typhi IgG antibodies
We measured IgG antibodies targeting HlyE, CdtB, and Vi antigens in serum from the 937 participants. Overall, the anti-Vi antibody titers ranged from 7.4 U/ml to 600 U/ml, the anti-HlyE IgG antibody titers ranged from 12.6 EU to 5163.2 EU, and the anti-CdtB IgG antibody titers ranged from 2.8 to 1466.1 EU (Table 2). Notably, 469/937 (50.1%) of the samples generated anti-Vi IgG titers that were below the calculation limit of 7.4 U/ml. The mean anti-HlyE, anti-CdtB, and anti-Vi IgG titers among all participants were 453.8 EU, 16.8 EU and 7.5 U/ml, respectively (Table 1).
Our data show a clear distinction between children and adult typhoid fever serology (Figure 1). Median anti- HlyE IgG and anti-CdtB IgG titer were higher in children than in adults (p<0.0001, Wilcoxon test). Median anti-Vi IgG titers were higher in adults than in children (p<.0001, Wilcoxon test).
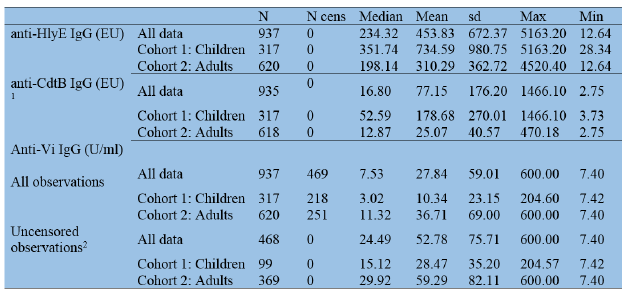
N = total number per group; N cens = number of observations below the calculation limit (censored values); sd = standard deviation 1Two participants whose samples were repeatedly below the calculation limit in the anti-CdtB IgG assay were excluded from the analysis 2Robust regression on order statistics were used to calculate summary statistics, due to the high number of observations below the limit of calculation
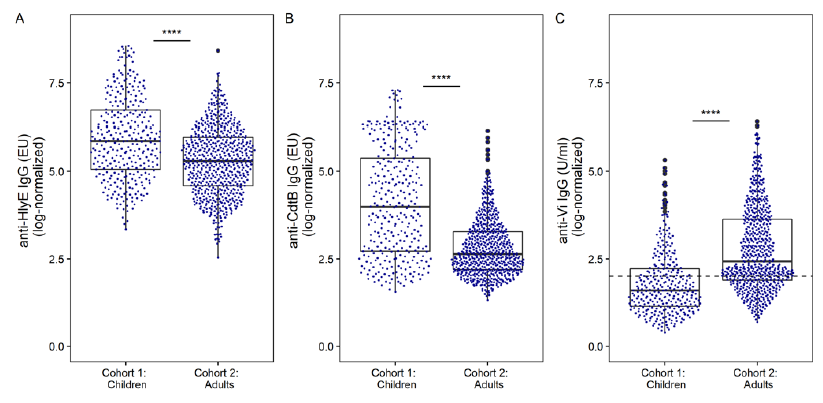
Figure 1. The distribution of anti–S. Typhi serum IgG titers in children and adults in Lao PDR Each dot shows the antibody titer of an individual sample for (A) anti-HlyE IgG, (B) anti-CdtB IgG, and (C) anti- Vi IgG with an underlying boxplot. The dashed line in panel C represents the censoring limit, all data points below were treated as left-censored data. Differences between groups were assessed using Wilcoxon rank sum test followed by Dunn’s post-hoc test with Bonferroni correction: ****p<0.0001.
The relationship between age and anti–S. Typhi serum IgG antibodies
In order to investigate the relationship between anti- HlyE IgG / anti-CdtB IgG and age, we fitted generalized additive models. The models suggested the highest antibody prevalences in children under 5 years of age and a decrease in antibody titers until the age of 20 years (Figure 2).
The anti-Vi IgG data was fitted as a function of age, which showed a positive relationship using Akritas– Theil–Sen non-parametric regression to account for the censored data; suggesting that anti-Vi IgG increases with age (Figure 2).
Trends in anti–S. Typhi serum IgG antibodies regarding sex, occupation, and location
There was no significant difference for any of the anti-S. Typhi antibodies between male and female children or adults. There were certain differences between occupation groups: Median anti-HlyE IgG titer were higher in office workers compared to students and compared to soldiers.
Median anti-CdtB IgG titers were higher in office workers compared to students and compared to soldiers. There were no significant differences in anti-Vi IgG titers between occupation groups.
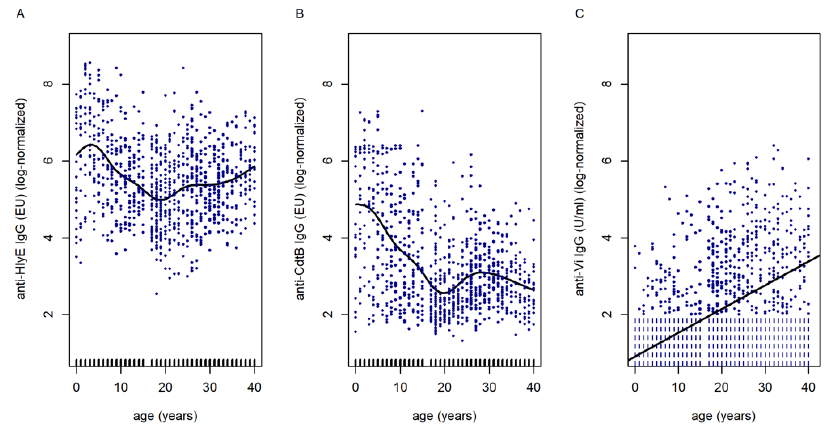
Figure 2. Results of generalized additive and linear models assessing anti–S. Typhi IgG antibody prevalence in children and adults in Lao PDR as a function of age. Non-linear smooths were fitted for age in the model for anti-HlyE IgG (A) and anti-CdtB IgG (B) data. The tick marks on the x-axis are observed data points. In panel C, the Akritas-Thiel-Sen regression line relating to the anti- Vi IgG titer data as a function of age was plotted in order to account for the censored values (censored observations were plotted as vertical dashed lines).
Discussion
In this study, 50.1% of the participants had anti-Vi IgG antibody concentrations <7.4 U/ml with an estimated median titer of 7.5 U/ml. Median baseline concentrations were higher in adults as compared to children (11.3 vs 3.5 U/ml) and a positive relationship of anti-Vi IgG titer and age was observed. The median anti-Vi titer without those measurements below the calculation limit was 24.5 U/ml in general and 29.9 U/ml among adults, which was higher than previously reported median titers of 8.6 U/ml and 21 U/ml in healthy adults from Spain and Germany (Sanchez-Ramon et al., 2016, Evans et al., 2018).
In contrast to the anti-Vi IgG data, the median anti-HlyE IgG and anti-CdtB IgG titers were higher in children than adults. The non-linear trend line fitted to the HlyE IgG data suggested a peak in concentration in children below 5 years of age, followed by a decrease and before increasing again after the age of 20 years. The anti-CdtB IgG data followed largely the same projection; however, an increasing trend after the age of 30 years was not observed.
This study offered the first insights into the age-related prevalence of three antibodies against S. Typhi. The prevalence of antibodies developed against the two protein antigens, anti-HlyE IgG and anti-CdtB IgG, indicates a high exposure in children. These findings are somewhat in contrast to a hospital-based surveillance study in Vientiane which reported no incidents of typhoid fever in children over the course of two years (Chanthavilay et a., 2020).
The results of this study have recently been submitted for publication.

COVID-19 serostudy. Study team (Institut Pasteur du Laos staff and students from Lao Tropical Public Health Institute), and participants holding study information sheets, outside a health centre in Oudomxay province.